Research Projects
Our research groups focus on a variety of neuro-research topics. Here are some summeries of the leading neuro-reasearch being done in our labs.
Alzheimer's Disease Research
"…Our research provides the first evidence in Alzheimer’s disease research that shows SCF+G-CSF treatment to have long-term effects in the recruitment of bone marrow-derived monocytes and macrophages (BMDMs)."
Li-Ru Zhao, MD, PhD
Professor
Expand to read more...
Long-term effects in the recruitment of bone marrow-derived monocytes and macrophages (BMDMs)
- Alzheimer’s disease (AD) is the most common cause of dementia and death, and it also represents a heavy financial burden in the United States. Effective treatments that can stop or slow the progression of AD have not yet been developed. AB deposition in the brain plays a crucial role in the development of AD. Bone marrow-derived monocytes/macrophages (BMDMs) have been proven to be critically involved in AB clearance in transgenic mouse models of AD. Clinical studies have revealed a low level of BMDMs in the blood and bone marrow of AD patients. Plasma SCF and G-CSF are also reduced in AD patients. The role of SCF and G-CSF in maintaining BMDMs and regulating BMDMs to remove AB in the brain of AD, however, remains unclear. Using bone marrow transplantation to track BMDMs, the Zhao Lab’s studies have provided the first evidence in the AD research field showing that SCF+G-CSF treatment has a long-term effect in recruitment of BMDMs into the brain and in the increase of AB clearance in an APP/PS1 mouse model. The findings of Zhao Lab have revealed that 9 months after SCF+G-CSF treatment, the number of BMDMs and the association of BMDMs with AB plaques are increased, and that AB deposition in the brain is reduced in SCF+G-CSF-treated APP/PS1 mice. In addition to dramatic reductions of AB load in the brain, SCF+G-CSF treatment in aged APP/PS1 mice also shows reduced neuroinflammation in the brain. These findings reveal the contribution of SCF and G-CSF in slowing the pathological progression of AD. This unique pharmacological approach offers a potential therapeutic strategy for AD. In a NIH/NIA-supported research project (1R01AG051674 to LR Zhao), the Zhao research team is exploring the underlying mechanisms of how SCF+G-CSF treatment delays the pathological progression of Alzheimer’s disease in transgenic mouse models.
Brain Tumor Research

"...Our laboratory is currently identifying and targeting the mechanisms by which glioma cells can escape immune responses."
Mariano S. Viapiano, PhD
Associate Professor
Mariano S. Viapiano, PhD
Associate Professor
Expand to read more...
Re-activating the Immune System to Attack Malignant Gliomas:
- Malignant gliomas are a formidable challenge for cancer therapies because these tumors are protected by an isolated, immunosuppressive environment in the Central Nervous System. Our laboratory is currently identifying and targeting the mechanisms by which glioma cells can escape immune responses. We have developed a novel antibody that blocks the extracellular matrix protein fibulin-3 and promotes an inflammatory reaction against the tumor. Our initial results (Nandhu et al., Clin. Cancer Res. (2018) 24:821-833) suggest that the antibody can boost immune responses against malignant gliomas and other types of aggressive solid tumors such as mesothelioma and renal cell carcinoma.
Innate immune cells (macrophages, blue) move towards a glioma in the brain (yellow cells, arrows); however, they are “hijacked” by the tumor and become immunosuppressed (M2 macrophages, magenta). Copyright source: Viapiano et. al. "Malignant Glioma Microenvironment". In: Youmans and Winn Neurological Surgery 7th Ed (2017).

"...In a new project, we are developing CAR-Ts against novel targets localized in the tumor microenvironment."
Mariano S. Viapiano, PhD
Associate Professor
Mariano S. Viapiano, PhD
Associate Professor
Expand to read more...
Engineering T-Cells Against the Tumor Microenvironment:
-
Engineered T cells carrying Chimeric Antigen Receptors (CAR-Ts) have shown impressive results against leukemias but still face significant obstacles to work against solid tumors. In a new project, we are developing CAR-Ts against novel targets localized in the tumor microenvironment. We have confirmed that these CAR-Ts are highly cytotoxic against tumor cells (Sengupta et al., Neuro-Oncology (2018) 20 (Suppl 6): vi129-vi130) and can be employed to attack glioblastomas and other solid tumors.
Malignant glioma cells in culture (green) shown alone or after 3 hours of co-culture with naïve T cells or engineered CAR-Ts against a tumor antigen. Notice the accumulation of CAR-Ts on the surface of the tumor cells.
"...Our laboratory investigates the mechanisms by which glioma cells proliferate and invade the brain in response to signals provided by glial cells."
Mariano S. Viapiano, PhD
Associate Professor
Mariano S. Viapiano, PhD
Associate Professor
Expand to read more...
Identifying New Mechanisms of Brain Cancer Resistance to Therapy:
- Malignant gliomas are supported by a unique repertoire of neural cell types that secrete tumor-promoting signals, favoring tumor growth and invasion. Our laboratory investigates the mechanisms by which glioma cells proliferate and invade the brain in response to signals provided by glial cells. Our goal is to identify key mechanisms that can be disrupted to “isolate” tumor cells from the supporting cells in the brain. We have recently demonstrated that extracellular matrix molecules secreted by tumor cells (but absent in normal brain) direct the behavior of glial cells (Nandhu et al., Oncogene (2017) 36:4875-4886) and can be targeted to reduce tumor growth.
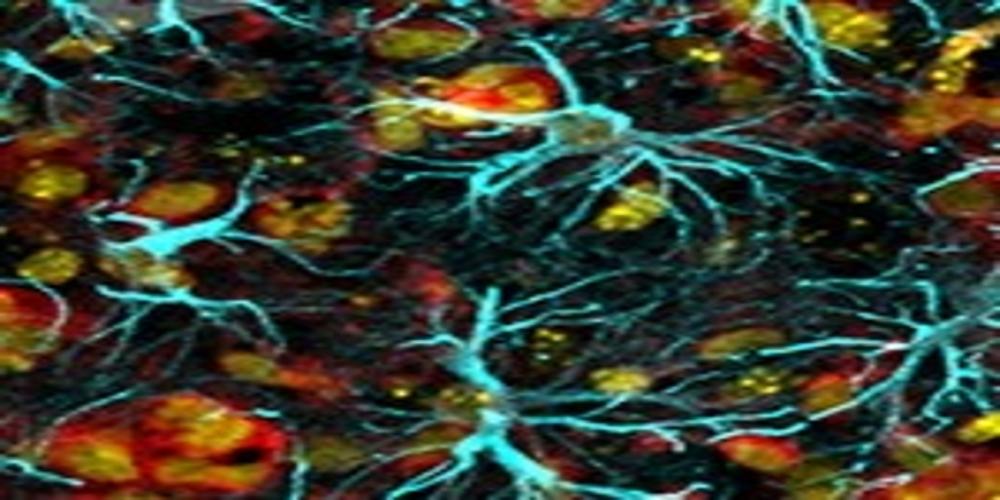
Tumor cells overexpressing the ECM protein fibulin-3 (fibulin-3 OE) promote astrocyte reactivity that enhances tumor growth. Cyan: astrocytes (GFAP); red: tumor cells (p65 NFkB ); yellow: tumor cell nuclei.
CADASIL Research
"…We are currently exploring the therapeutic approach for restricting the pathological progression of CADASIL."
Li-Ru Zhao, MD, PhD
Professor
Expand to read more...
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy
- Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is a Notch3 mutation-induced cerebral small vessel disease and represents the most common form of hereditary stroke and vascular dementia. It remains largely unknown, however, how Notch3 mutation drives the disease development. To date, there is no cure for CADASIL. The Zhao Lab is the first group to explore the therapeutic approach for restricting the pathological progression of CADASIL using a transgenic mouse model of CADASIL (TgNotch3R90C). In a long-term study, the Zhao Lab has demonstrated that repeated SCF+G-CSF treatments ameliorate CADASIL-associated pathology including cognitive impairments, vascular smooth muscle cell degeneration, cerebrovascular regression, neural progenitor cell loss, perivascular glycoprotein aggregation, and capillary thrombosis and leakage in the cortex. These data indicate that SCF+G-CSF treatment shows therapeutic potential in ameliorating pathological severity and restricting progression of CADASIL. In addition to revealing the unique pathology of cerebral cortical capillary thrombosis and neural progenitor cell loss, the Zhao Lab has also discovered the co-existence of reduced vascular endothelial growth factor (VEGF) and reduced blood vessels in the brains of TgNotch3R90C mice, indicating the involvement of VEGF in pathogenesis of CADASIL. Through mechanistic studies, SCF+G-CSF treatment-enhanced cerebrovascular regeneration through the upregulation of VEGF has been demonstrated to play a central role in promoting neural structural regeneration, synaptogenesis, neurogenesis and cognitive improvement.
- The CADASIL research project has been supported by American CADASIL Foundation and American Heart Association (15GRNT25700284 to LR Zhao). The ongoing studies in Zhao Lab aim to define how Notch3 mutation drives cerebrovascular dysfunction and how SCF+G-CSF treatment ameliorates Notch3 mutation-induced cerebrovascular dysfunction.
Traumatic Brain Injury (TBI) Research
"…We are exploring new therapeutic strategies for enhancing TBI recovery."
Li-Ru Zhao, MD, PhD
Professor
expand to read more...
Enhancing TBI recovery
- Traumatic brain injury (TBI) represents a public health crisis in the United States. The lack of treatment for enhancing post-TBI recovery, insufficient knowledge of post-TBI pathology, and the requirement of clinically relevant animal models are the major challenges in the field of TBI research. Exploring new therapeutic strategies for enhancing TBI recovery. TBI is not only an event that needs acute management, but it is also the onset of a chronic health condition requiring chronic treatment and care. Severe TBI causes lifelong disabilities and increases the risk of developing dementia, major depression and neurodegenerative diseases. It has even been known to cause death during the chronic phase. Recent major advances in acute medical and surgical management have dramatically increased the survival rate following severe TBI. As a result, the population of severe TBI survivors is increasing. However, an effective and evidence-based treatment for TBI recovery is not yet available. It raises a critical need, therefore, to develop treatment for improving functional outcomes for severe TBI survivors. Using a severe TBI mouse model developed in our lab (the Zhao Lab), we have demonstrated therapeutic efficacy of stem cell factor (SCF) in combination with granulocyte colony–stimulating factor (G-CSF) (SCF+G-CSF) in subacute TBI. This is the first study demonstrating the therapeutic potential of a pharmacological approach, SCF+G-CSF, to improve severe TBI recovery weeks after injury. In a VA-funded TBI research project (I01 RX002125 to LR Zhao), we have further determined the restorative efficacy of SCF+G-CSF in chronic TBI. Our findings have revealed that SCF+G-CSF treatment in the chronic phase of severe TBI (several months post-TBI) improves long-term functional outcomes, ameliorates severe TBI-induced widespread neuropathology, reorganizes neural structure networks, and promotes white matter remyelination. These studies demonstrate the therapeutic potential of a pharmacological approach, SCF+G-CSF, in enhancing severe TBI recovery in the chronic phase for the first time. Our ongoing studies are exploring the mechanisms underlying the SCF+G-CSF-enhanced brain repair in the chronic phase of severe TBI.
Revealing underlying mechanisms of TBI pathology
- Using the severe TBI model in young adult mice, we have also discovered a novel role of S100a9 in exacerbating TBI pathology and worsening post-TBI recovery. This study provides novel insight into the pathological involvement of S100a9 in TBI, which could offer a new therapeutic target to reduce brain damage after TBI. In a long-term time-course study, a unique profile of pathological progression has been observed in the severe TBI mouse model. This study sheds new light on pathological mechanisms of severe TBI progression.
Exploring chronic traumatic encephalopathy (CTE)
- Developing clinical relevance of animal models for chronic traumatic encephalopathy. Chronic traumatic encephalopathy (CTE) represents a progressive neurodegenerative disease associated with repeated closed head injury. This disease is characterized by progressive neuron death throughout the entire brain and is accompanied with cognitive decline and behavioral/mood abnormalities. The highest incidence of CTE is found in young professional/sub-professional athletes and military veterans. The lack of clinically relevant animal models for CTE creates an obstacle in improving the understanding of the pathogenesis of CTE and in developing therapeutic approaches to improve CTE recovery. To overcome this obstacle, our lab is working on developing a mouse model that recapitulates clinical CTE.
Stroke Research
"…We are exploring lifelong brain plasticity and demonstrating the long-lasting possibilites of reparing a stroke-damanged brain."
Li-Ru Zhao, MD, PhD
Professor
Expand to read more...
Improving stroke recovery and expanding research
- Stroke represents a severe medical condition that causes stroke survivors to suffer from long-term and even lifelong disability.
- Dr. Zhao has recently recognized and demonstrated that lifelong brain plasticity offers the long-lasting possibility of repairing a stroke-damaged brain. The window of restorative therapy for improving stroke recovery is much longer than previously thought, which lasts from years after stroke onset to lifelong. A stroke not only causes neuron loss in the infarct area but it also disrupts entire brain networks, resulting in widespread brain network dysfunction, which is not only limited to deficits in sensorimotor function but also causes impairments in recognition, and spatial and mood control function. Restorative approaches that contain multiple components to rebuild and normalize the stroke-disrupted brain networks and brain functioning, therefore, would be the next generation of therapies for enhancing brain repair and stroke recovery. The Zhao Lab is exploring this next generation of restorative treatments for maximally enhancing brain repair and improving stroke recovery in the chronic phase.
- The Zhao Lab has demonstrated the neurorestorative efficacy of SCF+G-CSF in chronic stroke using a stroke model created in spontaneously hypertensive rats (SHRs), which is the stroke model most relevant to the pathology of stroke patients. Initially, the permeability of SCF and G-CSF across the blood-brain barrier has been revealed, and the synergistic effects of SCF+G-CSF in promoting neurite outgrowth through the PI3K/AKT/NFκB/BDNF pathway have been clarified. Supported by these fundamental studies, the Zhao research team carried out a series of studies using a variety of approaches including molecular biology, cellular biology, 2-photon live brain imaging, neurobehavioral testing, and immunohistochemistry to determine the mechanisms underlying the SCF+G-CSF treatment-enhanced brain repair and functional outcomes in the chronic phase of experimental stroke. The research findings of the Zhao Lab have revealed that SCF+G-CSF-enhanced regeneration of axons, synapses and blood vessels in the chronic stroke brain are required for neurological function improvement. These studies were supported by NIH/NINDS (5R01NS060911 to LR Zhao) and American Heart Association (0865352E to LR Zhao).
Expand all
Anti-Angiogenic Targeted Toxins against Malignant Gliomas
Walter A. Hall, MD, Professor
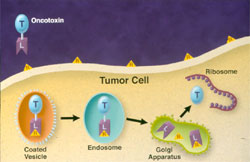
The prognosis for patients with glioblastoma multiforme (GBM) treated with conventional therapies remains poor. Glioblastoma multiforme is the most common brain tumor in adults and represents 40% of all brain tumors seen annually. One attractive alternative treatment is recombinant targeted toxin (TT) therapy. Targeted toxins are hybrid molecules containing a potent catalytic toxin and a carrier ligand that selectively recognizes the target tumor. After entry into the cancer cell, the TT will kill the cell by blocking protein synthesis (Figure 1). Although TT therapy has been around for a number of years, its use has been limited by organ toxicity when administered systemically.
Injection of the TT directly into the brain tumor will circumvent the problem of systemic toxicity. Brain cancer therapy affords the advantage of local intracranial delivery and clinical responses for this disease have far exceeded those for other cancers with reported response rates in excess of 50%. These encouraging results are mainly because localized delivery can concentrate therapy at the site of tumor diminishing the risk to nontarget organs. Another major advantage of using TT is their effectiveness against both dividing and non-dividing cancer cells in contrast to radiation therapy and conventional chemotherapy that are directed against dividing cells.
Past Clinical Trials
A group at the National Institutes of Health evaluated the toxicity of a TT called TransMID consisting of transferrin as the ligand linked to an altered form of diphtheria toxin (DT). A prospective trial with TransMID was conducted in 18 patients. To distribute TransMID in the tumor and into areas of the brain infiltrated with tumor, they used high flow microinfusion to establish interstitial convection and enhance distribution. Following a positive biopsy, one to three infusion catheters were placed in the tumor. Intratumoral infusions were well tolerated and therapeutic responses were observed. At least a 50% decrease in tumor volume occurred in nine of 15 evaluable patients.
Several other targeted toxins have been developed and tested in clinical trials. These include mutated forms of Pseudomonas exotoxin linked to proteins that targeted the interleukin-13 receptor, the interleukin-4 receptor, and the epidermal growth factor receptor. Only TransMID contains an altered DT. The results of these trials are presently being analyzed. Currently, there are no open clinical trials for TT therapy.
Future Clinical Trials
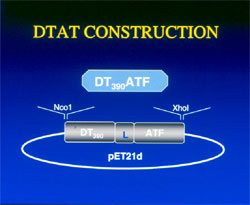
We have developed a TT against GBM for future use in early phase clinical trials. A recombinant hybrid fusion protein DTAT (Figure 2) was created using a mutated 390-amino acid portion of DT, a linker, and the non-internalizing 135-amino acid terminal (AT) fragment of human urokinase-type plasminogen activator (uPA). DTAT has the advantage over other fusion proteins of targeting the uPA receptor on malignant glioma cells and the endothelial cells of the neovasculature that supplies the tumor. The toxicity, specificity and efficacy of DTAT were evaluated in an intracranial model of human GBM.
The maximum tolerated dose (MTD) of DTAT was determined for three consecutive injections administered every-other-day and by convection enhanced delivery. Intratumoral injection of 0.15 mg every other day for 3 doses was performed in a murine intracranial U87MG GBM model. Convection enhanced delivery of DTAT in nude mice with established intracerebral U87MG brain tumors resulted in significant reductions in tumor volume and prolongation of survival in treated animals compared to controls (P < 0.0001). MR imaging was performed to evaluate the brain for neurotoxicity and the tumor for a therapeutic response. The total MTD for DTAT was 0.45 mg and the total MTD using CED was 5 mg. Toxicity was manifest as weight loss and cerebral infarction.
Experiments in uPA knockout mice revealed that toxicity was not receptor related. MR imaging demonstrated a marked decrease in tumor burden and no evidence of intracranial hemorrhage or vascular leak syndrome. DTAT is an active agent against intracranial GBM without demonstrating evidence of hemorrhage on MR imaging or neurotoxicity on histological examination. Toxicity studies are being conducted in a porcine model. These results support the further development of DTAT for future clinical trials in patients with GBM.
Figure 1. Mechanism of action for targeted toxins. After entry into the cytosol, they are transported in vesicles to the Golgi apparatus where the toxin is cleaved. The toxin will inhibit protein synthesis by preventing the addition of amino acids. Blocking protein synthesis kills the cell.
Figure 2. DTAT. Schematic of the plasmid for inserting the gene sequences into bacteria in order to produce the anti-angiogenic targeted toxin, DTAT.
Spinal Cord Injury
Spinal Cord Plasticity After Injury
Blair Calancie, PhD, Professor
In our laboratory of Clinical Neurophysiology, we have two primary interests: 1) spinal cord synaptic reorganization (i.e. plasticity) and regeneration after injury; and 2) intraoperative monitoring of CNS function during surgery.
Spinal Cord Plasticity after Injury
We use electrophysiological, functional, and kinematic measures to better understand the spontaneous (naturally-occurring) and therapy-related changes in brain and spinal cord function that occur after spinal cord injury (SCI). Much of our work is carried out on human volunteers, many of whom have sustained traumatic spinal cord injury. The information gained from these studies will help expand our understanding of the mechanisms underlying recovery from injury. From a practical viewpoint, this research may also help with subject selection and study effectiveness (i.e. through novel outcome measures we have developed) as our findings are incorporated into clinical trials of novel treatments for SCI.
Several projects in this area are currently underway in our lab. First, we are interested in quantifying the time course and extent of plasticity within the autonomic nervous system after acute SCI in humans, in order to study the basis for autonomic dysreflexia (AD). We typically begin studies within one week of each subject’s acute injury, repeating our measures over the intervening days, weeks, months, and years. Measures include blood pressure (real-time; noninvasive), cutaneous blood flow (laser doppler), and heart-rate variability in response to controlled afferent stimulation designed to mimic the earliest stages of dysreflexia. Our findings to date suggest that AD is a consequence of novel sprouting from afferent fibers lying caudal to a region of SCI onto partially denervated sympathetic preganglionic neurons lying within the thoracic spinal levels. We are also examining central motor conduction and the influence of repetitive, high-frequency transcranial magnetic stimulation (TMS) on brain excitability and muscle recruitment (via EMG). This project is funded through an R01 from NIH.
As many as 15-20% of persons admitted to the hospital with SCI have actually sustained damage to the nerve roots at the base of the cord (the cauda equina). Despite this relatively high incidence, attempts to repair nerve damage are rarely attempted, nor are there even animal models for this type of injury. In response, we have embarked on a multi-disciplinary project to develop and characterize a cauda equina injury model in the rat, and then treat damaged nerve roots with a combination approach involving implantation of a nerve conduit seeded with Schwann cells and nanospheres acting as molecular delivery agents for neurotrophins (e.g. GDNF) and anti-scarring agents. This project includes investigators from Syracuse University (Biomaterials) and from multiple departments within Upstate Medical University. Once we have demonstrated successful nerve root regeneration in the rat, our goal is to first translate this approach to a dog model, and ultimately take this method to the clinic for treating acute cauda equina injury. This project is funded by the New York State Department of Health.
In a recently completed and NIH-funded study, we looked at the role that different forms of rehabilitation play in the recovery of walking ability in persons with chronic (> 1 year post-injury) and neurologically-incomplete spinal cord injury. We compared 3 forms of therapy: 2 methods using body-weight support (support over a treadmill vs support over fixed ground) and comprehensive physical therapy. We found that nearly all subjects showed considerable improvements in gait and other functional tasks, regardless of the treatment they received. The biggest improvements were in balance and maximal walking speed. These results indicate that many persons with chronic, incomplete SCI have significant levels of ‘untapped’ movement capability that can be accessed through novel physical exercise.
Spinal Cord Injury, Recovery and Rehabilitation
Blair Calancie, PhD, Professor
Natalia Alexeeva, PhD, Assistant Professor
Intraoperative monitoring of CNS function during surgery
We have a long history of developing electrophysiologic tests for helping to prevent neurologic injury to the brain, spinal cord, and nerve roots during surgical procedures that place these structures at risk. We were the first group to publish a technique for monitoring pedicle screw placement in the lumbosacral spine, with a method that is now considered a standard of care in most major spine centers. We also were instrumental in gaining FDA approval of a device for noninvasive stimulation of the brain’s motor cortex during surgery, in order to monitor the motor evoked potential (MEP). This approach, approved by the FDA in August of 2002 and now in widespread use across the US, has been shown to help prevent spinal cord injuries during such procedures as correction of scoliotic deformity, and resection of spinal cord tumors.
We have recently initiated a new study to develop a reliable method for preventing medially directed errors in placement of screws into thoracic-level pedicles. The technique combines key elements of our lumbar pedicle screw and MEP protocols. A thoracic pedicle screw placed medial to the pedicle will enter the canal space, and could potentially compress and/or lacerate the spinal cord. Needless to say, the neurologic consequences of such a placement can be devastating. Preliminary findings from our first 5 subjects indicate the technique is working exceptionally well, and we are confident we have already prevented the misdirection of several screws.
A new area of research we are considering is to apply novel monitoring techniques for detection of cerebral ischemia during cardiac surgery. The incidence of cognitive decline following cardiac surgery can exceed 25% in some studies, yet few centers are actively working to detect these events – caused by air or fat emboli, for example – and intervene with neuroprotective measures. Our goal is to develop an animal stroke model and evaluate the ability of these monitoring techniques to recognize such events.
Finally, we have begun an investigation into the neurologic basis for the development of scoliosis. This work is preliminary in nature, and is a direct result of our work in the operating room environment, summarized above. We hypothesize that the pattern of nerve connections from motor cortex to the spinal cord is different in persons with scoliosis than that seen in persons without scoliosis. To address this possibility, we are: 1) using single-pulse TMS and fMRI to map motor cortex; 2) testing manual dexterity; and 3) quantifying expression of key pathfinding genes. All of these procedures assess in a direct or indirect way the anatomy and physiology of the corticospinal tract; we suspect that abnormalities of this pathway’s innervation of the thoracic spinal cord contribute directly to the development of scoliosis.
Intraoperative Monitoring of CNS Function During Surgery
Blair Calancie, Ph.D., Professor
Natalia Alexeeva, Ph.D., Assistant Professor
Intraoperative Monitoring of CNS Function During Surgery
We have a long history of developing electrophysiologic tests for helping to prevent neurologic injury to the brain, spinal cord, and nerve roots during surgical procedures that place these structures at risk. We were the first group to publish a technique for monitoring pedicle screw placement in the lumbosacral spine, with a method that is now considered a standard of care in most major spine centers. We also were instrumental in gaining FDA approval of a device for noninvasive stimulation of the brain's motor cortex during surgery, in order to monitor the motor evoked potential (MEP). This approach, approved by the FDA in August of 2002 and now in widespread use across the US, has been shown to help prevent spinal cord injuries during such procedures as correction of scoliotic deformity, and resection of spinal cord tumors.
We have recently initiated a new study to develop a reliable method for preventing medially directed errors in placement of screws into thoracic-level pedicles. The technique combines key elements of our lumbar pedicle screw and MEP protocols. A thoracic pedicle screw placed medial to the pedicle will enter the canal space, and could potentially compress and/or lacerate the spinal cord. Needless to say, the neurologic consequences of such a placement can be devastating. Preliminary findings from our first 5 subjects indicate the technique is working exceptionally well, and we are confident we have already prevented the misdirection of several screws.
A new area of research we are considering is to apply novel monitoring techniques for detection of cerebral ischemia during cardiac surgery. The incidence of cognitive decline following cardiac surgery can exceed 25% in some studies, yet few centers are actively working to detect these events — caused by air or fat emboli, for example — and intervene with neuroprotective measures. Our goal is to develop an animal stroke model and evaluate the ability of these monitoring techniques to recognize such events.
Finally, we have begun an investigation into the neurologic basis for the development of scoliosis. This work is preliminary in nature, and is a direct result of our work in the operating room environment, summarized above. We hypothesize that the pattern of nerve connections from motor cortex to the spinal cord is different in persons with scoliosis than that seen in persons without scoliosis. To address this possibility, we are: 1) using single-pulse TMS and fMRI to map motor cortex; 2) testing manual dexterity; and 3) quantifying expression of key pathfinding genes. All of these procedures assess in a direct or indirect way the anatomy and physiology of the corticospinal tract; we suspect that abnormalities of this pathway's innervation of the thoracic spinal cord contribute directly to the development of scoliosis.